
Certified Anesthesiologist Assistant (CAA) Salary by State: 2025 Data and Why the Numbers Are Complicated
Most people outside the anesthesia world have never heard of a certified anesthesiologist assistant (CAA), and the salary data tends to surprise them.
CAAs are master’s-prepared anesthesia providers who work within a physician-led Anesthesia Care Team, delivering anesthesia and managing patients across the perioperative period under the direction of a supervising anesthesiologist. Entry requires a competitive premedical undergraduate background, a rigorous graduate admissions process, and a national certifying examination. The profession is currently authorized in more than 20 jurisdictions, with new state-level legislation advancing each legislative cycle. The workforce currently sits at roughly 4,000 practitioners, a number that reflects where the profession is in its geographic expansion, not a ceiling on where it is headed.
A small, specialized workforce operating in high-demand clinical environments tends to command strong compensation. The data bears that out, though some of it is more reliable than others, and understanding where the inconsistencies come from is what allows a reader to identify which numbers are actually worth using.
The Data Problem (and Why It Matters)
A search for CAA salary data on general aggregator sites will return figures ranging from the low $40,000s to well over $300,000. That spread is not a reflection of actual market variation. It is a classification problem.
The Bureau of Labor Statistics (BLS) is the federal agency that tracks occupational wage data across the U.S. economy. It does not publish a dedicated wage dataset for certified anesthesiologist assistants because CAAs do not have their own classification in the federal occupational coding system. When salary aggregators search BLS data using the CAA category, they are redirected to physician assistant figures instead. Those figures reflect PA compensation, which is a different profession with a different market. To make matters more confusing, some aggregators pull data for anesthesia technicians, a role that requires far less training and carries salaries in the $40,000 to $50,000 range. When those numbers surface on a CAA salary search, they are the wrong profession entirely.
The most credible data sources for CAA compensation are built from the ground up:
Employer job postings tracked by job boards such as BagMask.com and GasWork.com, which compile actual salary ranges posted by hiring employers
Clinician-reported salaries from Marit Health, a salary transparency platform with 174 verified, anonymously submitted CAA salary entries
These two sources are methodologically different, which is exactly why their convergence is meaningful. Job postings reflect what employers are willing to put in writing and compete on. Peer-reported data reflects what CAAs are actually earning and willing to share. When those two numbers tell the same story, the signal holds.
Top 10 States for CAA Compensation
The table below is drawn from employer job postings tracked by BagMask.com through Q4 2025. These are dollar figures pulled directly from active listings, representing what employers publicly offered in the market during that period.
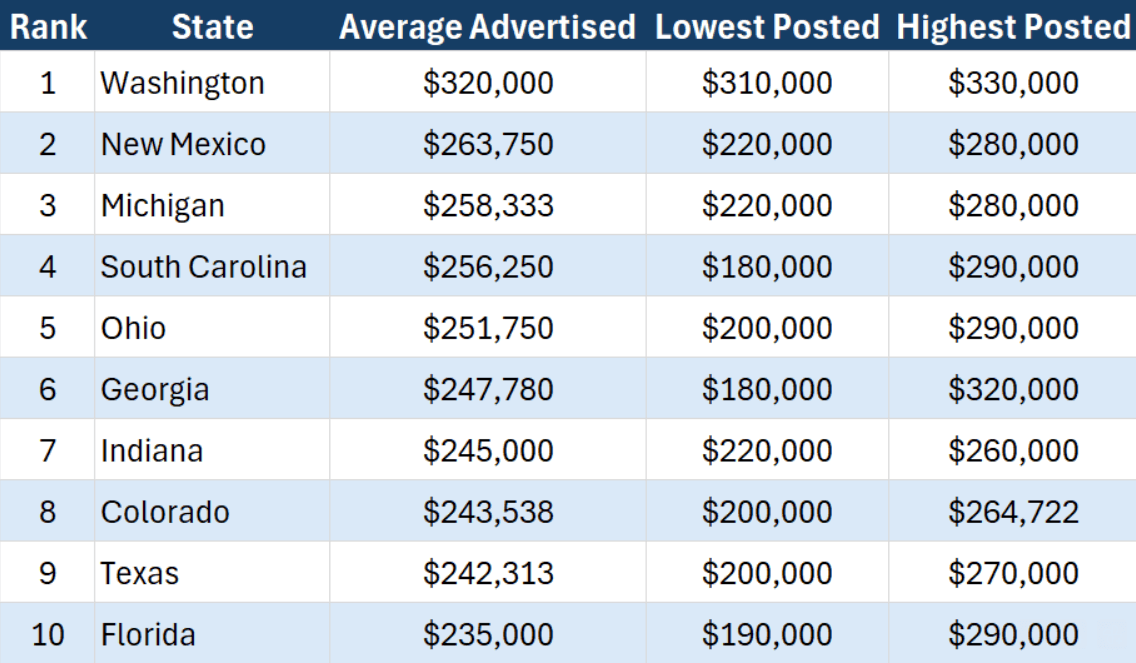
The numbers in the table are actual employer offers from active postings. Georgia’s $140,000 internal spread is a useful entry point for understanding why the same state can show such different figures.
Georgia presents the widest internal spread on the table, from $180,000 at the low end to $320,000 at the high end. That gap within a single state is not data error. It is the product of structural variation that is worth understanding, because the same kind of spread exists in other states too, just with a narrower range.
Why Salary Ranges Vary
CAA compensation varies because the roles that carry that title are genuinely different from each other in ways that matter. Three factors drive most of that variation.
1: Practice setting and case complexity
A CAA managing cardiac and transplant anesthesia at an academic Level I trauma center is not in the same market as a CAA providing anesthesia for routine outpatient procedures at an ambulatory surgery center. Both require advanced clinical training. The case complexity, procedural breadth, institutional infrastructure, and on-call demands are structurally different, and compensation reflects those differences. When a single state shows a six-figure internal salary spread, that spread almost always traces back to the range of settings represented across the postings.
2: Call structure
Overnight and weekend call carries premium compensation, and it should. It places real demands on a provider’s time and life outside the hospital, and that has a price. A position advertised at $280,000 with mandatory in-house call is a structurally different offer than one at $230,000 with no call obligations. Reading only the base salary number misses half the picture. The call structure tells you what was traded to get that number.
3: Geographic market maturity
CAAs can only practice in jurisdictions that have passed enabling legislation, and market development follows from there. States with years of authorized practice have built the infrastructure that makes hiring straightforward: employer familiarity with the role, established credentialing pathways, and competitive recruitment systems. Newly authorized states are starting from zero on all of that, and the salary data reflects two very different outcomes depending on where an employer falls on that curve.
Washington is the high-demand end of that spectrum. It authorized CAA practice in 2024 with strong institutional need and no existing local workforce. When employers have to recruit nationally for a role requiring specialized graduate training and national certification, compensation reflects that reality. The lowest advertised salary in Washington during Q4 2025 was $310,000. Other newly authorized states land at the opposite end: sparse posting activity, because institutions are still figuring out how to credential and hire for a role that is genuinely new to them. Same authorization status, opposite salary picture. The difference is institutional readiness.
Sign-On Bonuses and What They Add to Total Compensation
Sign-on bonuses have become standard in competitive anesthesia markets. BagMask data from 2025 shows active offers ranging from $50,000 to $100,000. Those numbers get attention, and they should. Understanding the mechanism behind them matters, because a sign-on bonus is not a gift.
A sign-on bonus is a retention mechanism. Employers offer an upfront lump sum in exchange for a contractual commitment to stay, typically one to two years. If a provider leaves before that period ends, the bonus or a prorated portion of it is subject to repayment. The structure serves the employer’s need for workforce stability in a market where qualified providers are scarce and recruitment is expensive. The bonus is compensation advanced against a promise to remain.
For the provider, the relevant questions extend well beyond the dollar amount. What triggers repayment? Is it prorated over the commitment period or is the full amount owed if the provider leaves at any point before the end date? Is the bonus paid as a lump sum at hire or distributed in installments? A $100,000 sign-on attached to a two-year repayment clause is a meaningful financial constraint on the ability to leave a position that turns out to be a poor fit, and it deserves evaluation as such.
With that context, total first-year compensation in competitive markets looks substantially different from the base salary alone. A $260,000 base with a $100,000 sign-on, retirement matching, CME allowance, and relocation assistance represents a total first-year value well above $400,000. In active markets, that kind of package is not an outlier. It is close to a standard offer structure.
What Top Earners Actually Make
The highest advertised base salaries for CAA positions in the United States currently cluster between $310,000 and $330,000, concentrated in Washington state and in specialized roles in Georgia. Emory’s cardiac anesthesia team was advertising $264,000 to $328,000 in 2025. ZipRecruiter’s 90th percentile figure for CAAs sits at $333,500, which aligns with what active postings show.
For CAAs working locum tenens, Marit Health’s peer-reported average rate is $215 per hour. At a full-time equivalent of 2,000 hours annually, that translates to roughly $430,000 before expenses. Locum work carries different trade-offs than permanent employment: variable scheduling, no employer-sponsored benefits, self-employment tax obligations, and frequent travel. For CAAs who pursue it strategically, it represents the upper range of what the profession pays.
CAA Compensation in Context
Robust salary data for CAAs is harder to find than it should be. The workforce is small, the BLS data gap is real, and the profession has not yet attracted the kind of large-scale compensation surveys that exist for other clinical roles. What exists are employer postings, peer-reported figures, and the information that circulates within the professional community. That is what this analysis is built on, and it tells a consistent story even with those constraints.
The profession is still completing its geographic footprint, with legislative campaigns advancing in multiple states each cycle. The workforce grows incrementally because authorization itself is still expanding, one jurisdiction at a time. The supply-demand dynamics behind these salary figures are structural, and they are unlikely to shift quickly.
For any healthcare professional mapping financial trajectory across career options, CAA compensation belongs in that analysis. The floor is higher than most people outside the profession realize. The ceiling reflects a market that has consistently priced specialized anesthesia skill at a premium.

Join the Newsletter
Stay up to date on pre-CAA content!

Sarah is a certified anesthesiologist assistant practicing at a Level I trauma center in Savannah, GA. She is the founder of Aspiring CAA, a clinical preceptor, and an author. With experience as a program admissions reviewer and a background in CAA education, she helps prospective students understand the path into the profession.
Salary data sourced from BagMask.com Q4 2025 advertised salary report, GasWork.com, and Marit Health clinician-reported salary data (174 verified CAA submissions, marithealth.com).
Popular posts
What is a certified anesthesiologist assistant and is it right for me?
By Sarah Whitfield on October 6, 2023
By Sarah Whitfield on October 17, 2023
Balancing CAA school with family responsibilities
By Sarah Whitfield on December 4, 2023
3 Anesthesia terms to know before shadowing a CAA
By Sarah Whitfield on October 9, 2023
By Sarah Whitfield on December 7, 2023
Who should write my CASAA letters of recommendation for CAA school?
By Sarah Whitfield on November 22, 2023
About this site
Aspiring CAA is the go-to blog for expert advice on how to become a CAA. Founded by a practicing certified anesthesiologist assistant with extensive experience as an educator and former admissions committee member, Aspiring CAA provides aspiring anesthesiologist assistants with valuable guidance. Drawing on the founder's deep knowledge of the admissions process, the blog simplifies applying to CAA programs and empowers applicants to succeed.


© Aspiring CAA